

Meets Luxury

Why Choose NOVA Plastic Surgery and Dermatology?
Over a decade ago, board-certified plastic surgeon Fadi Nukta, MD, had a vision. He wanted to create a medical aesthetic practice with a skilled, compassionate staff and effective treatments that would surpass patient expectations. In the years since, our practice has met and exceeded that goal.
Whether you are just starting to consider cosmetic treatments or have struggled with aesthetic concerns for many years, our goal is to educate you about your options and provide treatments that enhance the way you look and feel.

Top Plastic Surgeons in Northern VA, Nationally Recognized Physicians Assistants and Master Aestheticians
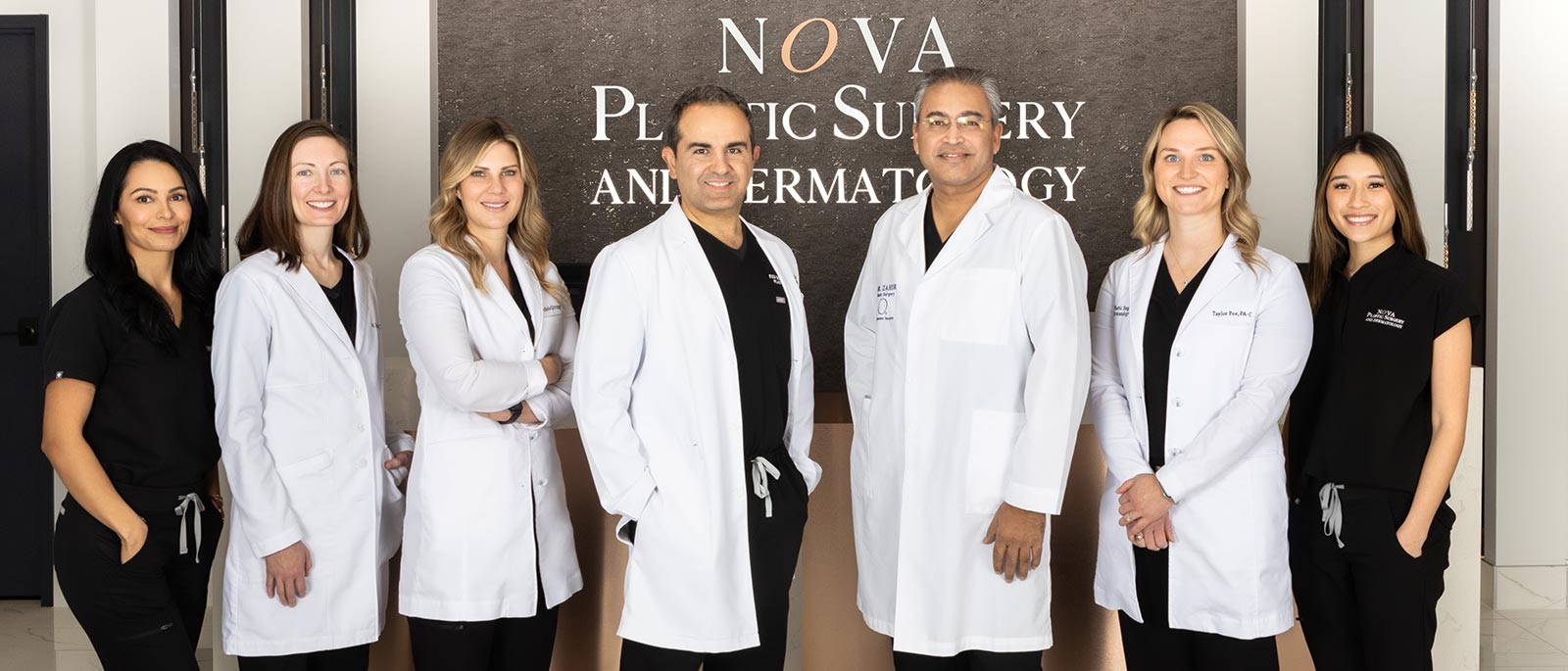
The heart and soul of NOVA Plastic Surgery and Dermatology is truly our team of experienced practitioners and staff members. Whether you’re engaging with a physician’s assistant or our office manager, we believe that every interaction with a customer should begin a trusting relationship that will stay for time to come.
Meet the Team
Breast Augmentation
Breast augmentation can enhance the size and shape of your breasts with implants. This cosmetic surgery is highly customizable to meet your desires.
Tummy Tuck
Tummy tuck surgery removes unwanted fat and skin from your abdomen and corrects abdominal muscle separation for a flatter, more toned stomach area.
Dysport®/BOTOX® Cosmetic
Dysport® and BOTOX® Cosmetic are injectable neuromodulator treatments that reduce and prevent wrinkles in your upper face, such as crow’s feet and frown lines.
HydraFacial MD®
HydraFacial MD® washes away contaminants from your skin, removes dead skin cells, and rehydrates your skin with unique moisturizers and antioxidant solutions.
Facial Fillers
Facial fillers are injectable treatments that reduce wrinkles and replace lost volume in your face. These treatments can smooth the skin and restore a more youthful shape to your face.
PRP for Hair Loss
Using natural growth factors in your blood, platelet-rich plasma (PRP) treatments can help restore hair follicles that have been lost to balding.
State-of-the art services, exceptional results, and an atmosphere that will leave you wanting.
View Services
Follow NOVA Plastic Surgery on Instagram
@novaplasticsurgery






Financing Available
We are pleased to offer interest-free financing. So do not let one lump sum payments get in the way of you getting the treatments you want. Inquire about our 6, 12, and 18 months interest-free payment plans.
Our Surgery Center
Are you ready to come for a consultation in the office? Great, we can schedule one with one of our experts. Alternatively, we can schedule virtual consultations from the comfort of your home.

SkinCeuticals SkinLab™
We have partnered with SkinCeuticals to create SkinLab™ NOVA. SkinLab™ is dedicated to bringing our patients top-level aesthetic medical experiences under the care of our Master Aestheticians and certified Physician Assistants. By combining top-of-the-line medical-grade skincare products with time-tested aesthetic treatments, SkinLab™ NOVA is here to help provide optimal skin health results.
Reviews From Our Patients
“I am 5 weeks post surgery and along with the professionalism and warm interaction I have received from the NOVA Plastic Surgery staff, Dr. Nukta’s work is absolutely spectacular. I could not be more happy with the results.”
“I’m so glad I found this place instead. Dr. Zahir was very knowledgeable during the consultation and quick and comforting during the procedure.”
“Throughout numerous surgeries and office visits, Dr. Nukta and Jenn have provided us not only with the very best medical care, but with a level of caring and compassion that we have never experienced with any other medical provider.”
“I am most satisfied with all the great care I received from Dr. Nutka and his fantastic staff. I would definitely recommend him to my family and friends.”
“Dr. Zahir confident and knowledgeable. He was an excellent surgeon and made me feel comfortable right away. They took great care of me at every visit and explained everything thoroughly.”
“All my friends compliment me and tell me how natural they look and always say what a great job the surgeon did. I have been recommending Dr. Nukta to all of my friends, and I highly recommend him to anybody considering breast augmentation!”